Obstetric forceps are medical instruments used to assist vaginal delivery.
As you can see in this modern forceps image (above right), obstetric forceps consist of 2 metal pieces that slot together, each consisting of a blade and a handle.
Forceps are rigid stainless steel instruments. Their metal construction makes them very durable and they are rarely discarded from hospital birthing units.
2. What did Medieval Forceps Look Like?
Obstetric forceps were first used in the 16th Century. They were invented by the Chamberlen family of obstetricians to avoid infant and maternal mortality during childbirth.1
Here is an image (right) of the Chamberlen forceps from 1580. (Courtesy of Wikimedia)
The basic forceps design remained largely unchanged throughout the 20th Century.
You can clearly see the strong resemblance to modern day forceps!
3. How are Forceps Used?
Forceps are used to guide the foetus (unborn baby) through the vagina (birth canal).
When the woman’s cervix is fully dilated (opened) the forceps blades are inserted through the vagina one at a time and locked in position around the foetal head. The forceps handles are then grasped to traction and guide the foetus out of the vagina.
An episiotomy (incision/cutting of tissues between anus and vagina) may accompany forceps delivery.
Let’s be clear on this issue; forceps are definitely indicated in some circumstances e.g. when vacuum extraction can’t be used in some medical conditions or stillborn deliveries. In some low resource, low income countries e.g. Africa, vacuum is not available and forceps save the lives of many.
However, both the rigidity and size of current obstetric forceps design may contribute to tearing of the pelvic floor muscles, nerves and supporting tissues during delivery.
According to Professor Peter Dietz pelvic floor damage occurs in approximately 44% of forceps deliveries and the use of forceps is currently on the rise in some Australian hospitals.3
4. What is the Current Size of Obstetric Forceps?
Ismail et.al.2 investigated the dimensions of 100 pairs of the most commonly used forceps in the UK (Neville Barnes’ and Wrigley’s forceps).
To show you the size of forceps, I’ve mocked this image from the manufacturer specifications for dimensions in results of this study.2
Just in case the numbers seem meaningless (which they were initially to me), here is the same image below with the real obstetric forceps size represented using standard size tennis balls where the foetal head is grasped. For the sake of accuracy, 3.7 tennis balls fit between the blades of these forceps.
This is the part of the rigid instrument that is withdrawn through the vagina once locked in place. There’s little wonder there is so much potential for prolapse after childbirth and beyond!
5. Lack of Forceps Manufacturing Standards
Of major concern is that manufacturers can currently vary the dimensions of the forceps they produce owing to the lack of official government prescriptive guidelines.
This means that while manufacturers must comply with general government industry guidelines for designing obstetric forceps, in many countries including USA, Australia and the UK2 the manufacturers can use their own specifications for the dimensions of the forceps they produce.
Manufacturers currently determine the dimensions/size of the forceps they produce.
There are currently no set government regulated prescriptive dimensions for forceps manufacture.
This means that obstetric forceps made by different manufacturers vary in size.2
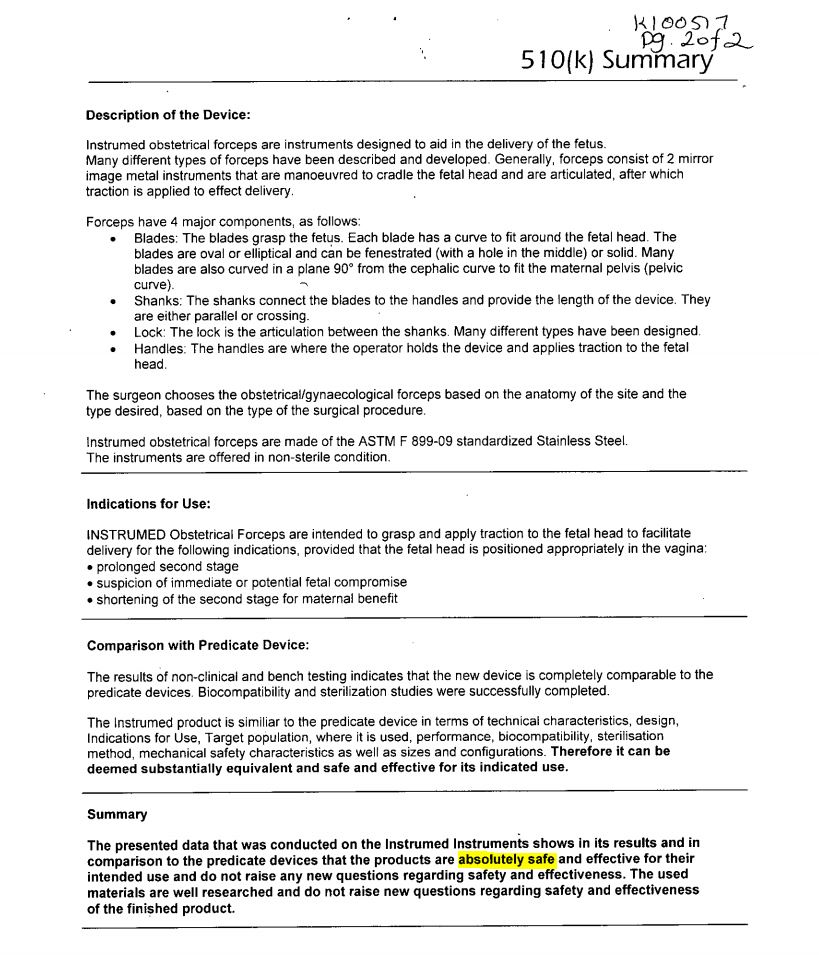
I would like to draw your attention to the “Description of the Device” which lacks any reference to size of instrument and the FDA approval safety “Summary”.
Click to enlarge
6. How can Technology Improve Forceps Design?
We now have new medical technologies that were never dreamed of in the middle ages!
To improve forceps design and reduce birth trauma here are a few suggestions …
Instant 3D printing of single use forceps2
– Why not have a set of appropriately sized single use forceps at the ready for a woman at high risk?
Medical imaging to measure the size of the female pelvisbefore delivery
Medical imaging of neonatal head sizebefore delivery
Modern materials (e.g. plastics) that allow single use disposable forceps
Implement government specifications for consistencyin forceps dimensions by manufacturers before approval is given by the relevant therapeutic body i.e. TGA (Australia), FDA (USA) and European Union
How Obstetricians Can Help Improve Forceps Design?
Obstetricians and medical caregivers are frequently placed in a very difficult position in relation to the use of forceps due to:
Pressure from hospitals to reduce c/section rates and opt for vaginal delivery
Pressure from expectant mothers who want a ‘natural’ delivery
Rising maternal age and obesity driving the rate of forceps deliveries3
Obstetricians can help by:
Demanding that manufacturers improve the current outdated forceps design
Lobbying for the introduction of single use 3D printed forceps
Identifying their patients at risk of protracted labour
Discussing the risks of protracted labour before labour begins
Taking a proactive approach by providing medical imaging of ‘at risk’ women and neonates prior to delivery
Yes we need to ensure that our obstetricians are proficient and highly trained in the use of forceps and perhaps some women need to be more flexible in their birth planning when it comes c/section versus vaginal delivery too.
Isn’t it time to move forceps design out of the middle ages?
Obstetric forceps 16th Century – 21st Century RIP
Have you had a forceps delivery? Have you experienced problems as a result of forceps?
1 Sheikh, S., Ganesaratnam, I., & Jan, H. (2013). The birth of forceps. JRSM Short Reports, 4(7), 1–4. http://doi.org/10.1177/2042533313478412
2 Ismail, A., Qader, T. & Ismail K (2016) Exploring variation in dimensions of obstetric forceps European Journal of Obstetrics and Gynecology and Reproductive Biology , Volume 198 , 170 – 171
Pelvic floor exercises for women in 3 simple steps for beginners with Pelvic Floor Physiotherapist Michelle Kenway. This Physiotherapist guided video teaches you: Pelvic Floor
Anal fissure treatment for anal fissure healing and relieving anal pain with bowel movements presented by Pelvic Floor Physiotherapist Michelle Kenway. Watch this video and
Proctalgia Fugax exercises and treatments at home can quickly relieve sudden onset anal pain. Proctalgia Fugax is thought to involve temporary spasm of the pelvic
Tailbone pain relief for sitting and healing coccydynia with Physiotherapist Michelle Kenway. Learn 4 cost effective ways to relieve tailbone pain with sitting and promote


 1")